Apply for the Award
| Site: | AMEE Learning Hub |
| Course: | ASPIRE submission home |
| Book: | Apply for the Award |
| Printed by: | Guest user |
| Date: | Wednesday, 17 June 2026, 10:31 AM |
Description
Award Information
This section contains further detail about the ASPIRE 'Curriculum Development' Award.
Please take the time to go through this content thoroughly to familiarize yourself with the application criteria and the expert panel involved in the process. Understanding these elements is crucial for a successful application.
At the end of the content, you will need to fill out the web form to generate the invoice. Completing this form is an essential step in your application process, as it will allow you to proceed with the payment for your selected award. Make sure to provide all the required information to ensure a smooth and efficient processing of your request.
To navigate, use the 'next' and 'back' arrows at the side of the page, or use the Table of Contents to jump to a specific page.
You can also download pdf versions of this guidance and a sample application form for reference.
About the Award
A curriculum is a statement of the intended aims and objectives, experiences, outcomes and processes of an educational programme (Grant, 2006).
A curriculum describes all the ways in which a training or teaching organisation plans and guides learning. This learning can take place in groups or with individual learners. It can take place inside or outside a classroom. It can take place in an institutional setting like a school, college or training centre, or in a village or a field. It is central to the teaching and learning process (Rogers and Taylor 1998).
Scope
For the purposes of this application, by “curriculum” we are referring to that which leads to the award of a primary medical, dental or veterinary qualification. An applicant institution or organization may have a single curriculum (e.g. one programme in medicine or dentistry or veterinary medicine) or more than one curriculum (e.g. one programme in medicine and one in dentistry or one in veterinary medicine; or two entirely separate programmes in medicine e.g. one for school-leavers and one for graduates). A separate submission must be made for each application.
Cultural, geographic, social, fiscal and other issues may influence how healthcare education is developed and delivered at an institution and will vary among institutions. Excellence may be identified and recognized in institutions with limited resources just as much as in “resource-rich” institutions. The way in which institutions demonstrate context appropriateness will be taken into account by the panel when reviewing each submission.
The focus of this ASPIRE award is on curriculum development, not primarily on the curriculum itself (although inevitably that has to be considered as part of the evaluation of its development).
Conceptual Frameworks
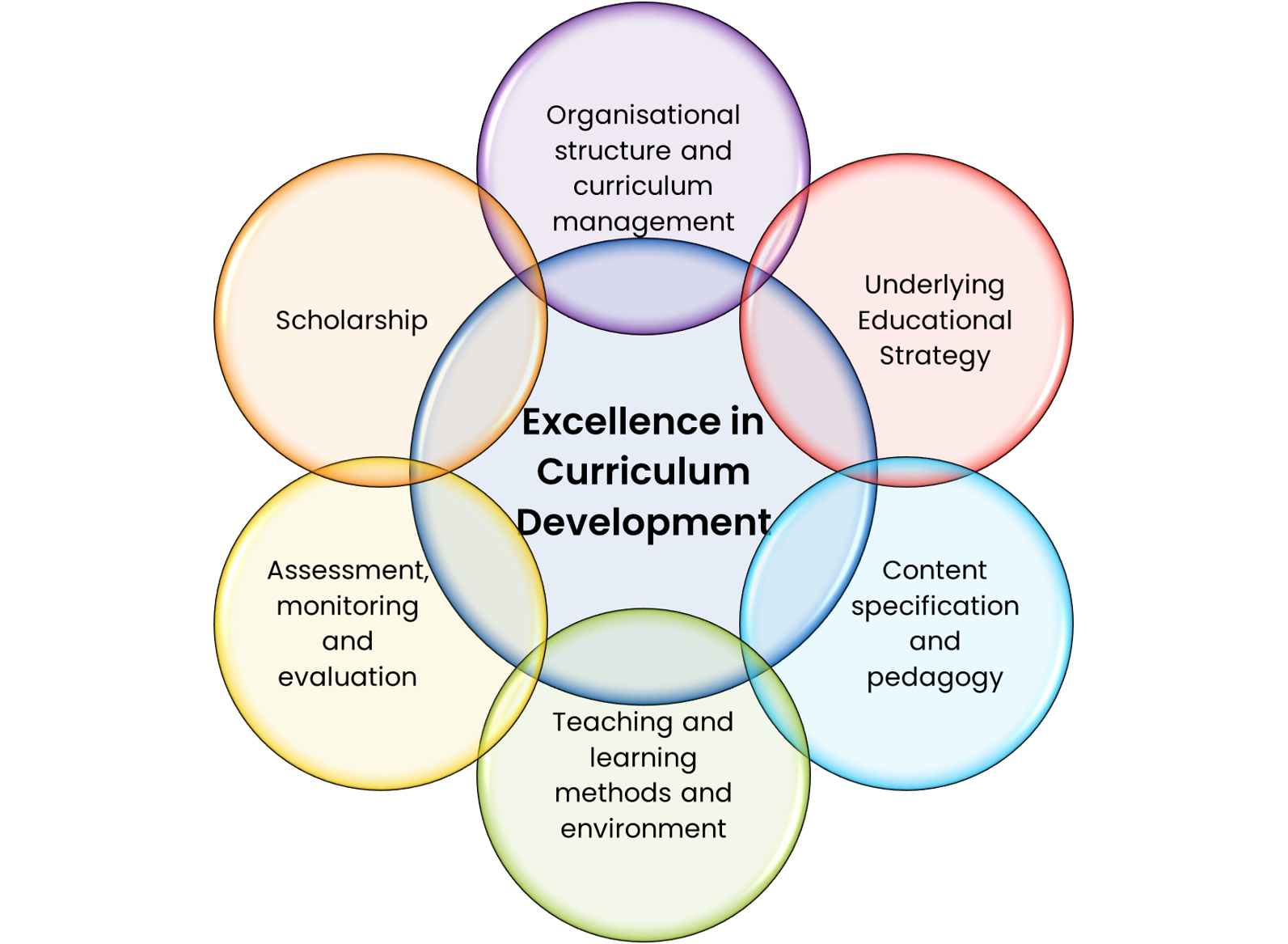
Excellence in healthcare curriculum development may be seen as the product of six components:
- Organisational Structure and Curriculum Management
- Underlying Educational Strategy
- Content Specification and Pedagogy
- Teaching and Learning Methods and Environment
- Assessment, Monitoring and Evaluation
- Scholarship
This framework will be used to map the criteria of excellence in healthcare curriculum development to continue to facilitate institutions to “aspire” and achieve excellence.
Expert Panel
- Sharon Peters (Co Chair) Canada
- Harm Peters (Co Chair) Germany
- John Jenkins, (Past Chair) Ireland
- Toh Chooi Gait, Malaysia
- Ming-Jung Ho, USA
- Janusz Janczukowicz, Poland
- Peter McCrorie, Cyprus
- Liz Mossop, UK
- Gustavo Quintero, Columbia
- Anne-Marie Reid, UK
- Indika Karunathilake, Sri Lanka
Prospective applicants are strongly encouraged to contact the panel chair for an informal discussion before beginning their application. The examples provided by the reviewers are shown below under the respective criteria. These examples are intended to be indicative and not exhaustive. You may have other evidence that would be equally important and which support your case for excellence.
Application process
All applications must be submitted online, but you are encouraged to download a copy of the application form and review the information that's required. This includes information about the submitters and their institution, opportunities for demonstrating excellence for the seven criteria and signatures of the lead submitter and the Head of the Institution. Before addressing the criteria, applicants are asked to provide an outline of the curriculum in diagrammatic form.
The institution’s designated programme will constitute “the curriculum” for the ASPIRE program application and the process of development of this curriculum will be assessed using the specified criteria for excellence.
The following pages provide detailed guidance on how to complete the application form for the curriculum development award. Included are:
- Descriptions of the types of evidence that should be provided as supporting documentation
- A glossary of key terms
Please read this document carefully to determine whether you meet the criteria for this award.
The Application Form
The application form contains 6 sections:
- Section A Submitter Information
- Section B Response Relating to Criteria
- Section C Summary
- Section D Additional Information / Supporting Documentation
- Section E Student Perspective
- Section F Certification Signatures by Lead Submitter and Dean of Institution
Each of these sections must be completed in full.
General Guidance
Responses to each criterion need to be specific and provide the evidence necessary to support the statement. Examples should be given where the curriculum development has had an impact.
It is recognised that cultural, social and other issues are likely to have an influence on the development and delivery of curriculum in an institution and that it will vary from institution to institution. Excellence may be found in institutions with limited access to resources just as much as in resource-rich institutions. The way in which institutions demonstrate the effectiveness of their programme within their particular context will be taken into account by the panel when reviewing individual submissions.
Language
The entire form must be submitted in a machine-readable format. All references to external documents or web sites must be via hyperlinks. With the exception of the appendices, all documentation should be in English. Where the appendices are in another language, a supporting commentary must be provided in English (see Commentary to Appendices below).
Glossary
A glossary of the key terms used in curriculum development is included at the end of this booklet.
Word limits
The expected word limit for each section is clearly stated within the form. It is important that these word limits are adhered to, and that the number of words used is indicated in the box provided.
Missing information
If a criterion or sub-category is considered not to be applicable to the institution, this should be stated on the form and appropriate justification provided.
Appendices
Where additional evidence is provided in the appendices, it must be made clear how the evidence demonstrates that the criteria have been met by the institution.
The appropriate section of the appendix should be identified and cross-referenced to Section B in the application form, making clear how the evidence is relevant.
All appendices should be numbered and listed in Section D of the form as Supporting Documentation.
The maximum number of Appendices permissible is 30.
Commentary to appendices
Each piece of supporting documentation included as an appendix must be accompanied by a short commentary in English to explain the relevance of the document and how it supports the institution’s statement. It should be clearly indicated which criterion or criteria are supported by the evidence in the appendix. The commentary should be no more than 300 words and summarise the key points from the appendix, including how the appendix provides evidence to support the statements in the submission document.
Please note: Evidence in an appendix that is not accompanied by a short commentary will not be reviewed.
Criterion 1
Organisational Structure and Curriculum Management
Key to any curriculum development strategy is having the right organisational management structure. Centralised management and committed leadership are both essential for effective change. Decision making must be clear and effective, while allowing for, and encouraging, the involvement of enthusiastic faculty at all levels. All stakeholders, both internal and external, should have some role in curriculum change.
Please tell us how the curriculum, and more specifically curriculum change, is managed in your institution, including the involvement of key stakeholders.
Examples of Evidence
- Provide an annotated diagram showing how the curriculum is managed, clearly listing the curriculum committees involved.
- Outline the major responsibilities of each committee, explain how they interact and state to whom they are accountable
- Describe the extent of any recent curriculum change e.g. piecemeal, partial, radical.
- Explain what triggered the change and describe how it was developed and implemented.
- List all stakeholders (by classification), both internal and external, who are involved in any way in curriculum development, curriculum management or curriculum evaluation, and briefly describe their involvement and their value to the change process.
- Outline how your institution provides resources for curriculum development, in terms of development costs, staffing, consultancy costs, equipment and facilities costs. (Note: actual costs are not required).
Criterion 2
Underlying Educational Strategy
In bringing about curriculum change and renewal, key to its success is having a clear educational strategy, and sound reasons for adopting this strategy.
There are three levels or stages in the development of a well-structured curriculum:
- The underlying education theory (epistemology) which results in the chosen educational strategy.
- How this has been translated into the content of the programme and the educational approaches (pedagogy) chosen for its delivery.
- The teaching and learning methods and environment in which they are delivered.
Examples of evidence
- Outline your educational strategy. Explain why you have adopted it, the theoretical framework underpinning it, and why it is appropriate for your school and region in terms of, for example, the vision/mission of your university or school, meeting the health needs of society (local, national or global), meeting accreditation standards, producing doctors skilled in clinical research or producing doctors trained to work in rural communities.
- Please provide evidence that the programme aims and outcomes to be achieved at the end of the programme are well defined and align with the overall educational strategy.
- Please outline any role played by national and/or international bodies in defining the outcomes or any other external guidance that was taken into consideration.
- Please describe the educational model that you use (e.g. discipline-based, system-based, module-based, theme based, spiral), demonstrate how it permeates the curriculum and explain the reason for adopting the model.
Criterion 3
Content Specification and Pedagogy
It is key to the design of any curriculum to have a clear understanding of what the students will be able to do upon graduation. This will be determined by the content of the programme and the educational approaches used in its delivery.
Please explain the rationale for the selection of the content of the programme and the educational approaches you have taken re its delivery. Please provide examples and evidence of excellence, where appropriate.
Examples of evidence
- Describe the extent to which the programme is integrated both horizontally and vertically (see glossary).
- Outline any vertical themes or strands which run through the programme and explain how they operate.
- Explain how you ensure that cognitive integration (see glossary) takes place for the learners and that it is not merely a timetabling exercise.
- Describe any interprofessional learning in the programme, including the nature of the interaction, which healthcare professionals and/or students are involved and what the level of interaction is. Outline how you promote teamwork in any other way, whether interprofessional or otherwise in your programme.
- Outline how student-centred your programme is. Describe the types of student-centred learning activities used in the curriculum. Please give some examples e.g. Case/Problem/Team Based Learning (see glossary for definitions). State how much student choice there is in your programme e.g. electives and selectives. Please give examples of particularly innovative projects that students have been involved in.
- Describe the extent to which your curriculum involves learning from real, simulated, virtual or paper-based patients. In particular, please explain how often and where students interact with real patients during the early years, outlining the nature of the interaction and explaining its purpose.
Criterion 4
Teaching and learning methods and environment
The teaching and learning methods should be appropriate for the nature of the material to be learnt – knowledge, skills or professional attitudes (e.g. as reflected in behaviour).
Please outline what teaching and learning methods you have chosen to use in your programme and explain the rationale behind your choice.
Examples of evidence
- Describe the rationale for choosing your teaching/learning methodology for the various aspects of the programme (e.g. knowledge, skills and professional attitude/behaviour)
- Outline how much clinical learning takes place in hospitals, clinics and in the community at each stage of the programme. Explain what the students gain from each setting. Indicate if students are exposed to clinical experience in other countries. If so, please describe how this is incorporated into the curriculum.
- Describe if e-learning is incorporated into your curriculum. If so, please explain why and how it is used and provide any evidence of its effectiveness. If there is no e-learning in your school, please explain the reason for this.
- Comment on the student learning environment, including learning spaces (library, study rooms, practical laboratories, skills laboratories, anatomy study areas, lecture theatres, tutorial rooms). Explain how an appropriate learning climate is created, how the safety of the learner is protected, how their respect is maintained and how they are protected from intimidation and harassment (from peers, faculty staff etc.)
Criterion 5
Assessment, monitoring and evaluation
Assessments must be directly related to learning outcomes, be reliable, be subjected to a rigorous quality assurance process, and be accompanied by a timely feedback process. The curriculum must also be subject to a quality assurance process, whether or not a new development or innovation has taken place. Feedback should be obtained from all stakeholders, action taken based on the findings and these actions fed back to the stakeholders.
Please outline your assessment strategy, describe the types of assessment you use and provide a rationale for your choice. Outline your process for curriculum monitoring and evaluation.
Examples of evidence
- Outline the process by which assessment is matched to learning outcomes. Please provide a sample blueprint of (a) a written examination and (b) a clinical assessment which demonstrates the link between assessment and learning outcomes. Explain how you assess clinical attachments, projects & electives and professionalism.
- Outline your policy for both formative and summative assessment feedback to students, including timeliness. Can you provide any evidence that assessment has promoted learning?
- Outline the methods you use for validating your assessments. Describe any external review of your assessments (if applicable).
- Explain how your curriculum is monitored and evaluated, by whom and how frequently. Explain the process for reviewing these evaluations. Summarise any findings from the evaluation and indicate any modifications to your curriculum that have taken place as a result of evaluation (Quality Improvement).
- Provide evidence that the findings from the evaluations are fed back to those who supplied the feedback (closure of feedback loop). Please also indicate if you refer to any external and more objective methods of evaluating the outcomes of your curriculum (e.g. examination results, performance of your graduates in the workplace, their career choices and practice patterns and their contribution to the workforce).
Criterion 6
Scholarship
Scholarship is important in any institution’s mission. This can take many forms, not just research and publications. To qualify for excellence in curriculum development, there must be evidence of achievement of scholarship.
Please tell us how your institution supports scholarship, including rewards for faculty engaged in scholarly activities. Note that it is not essential to have an extensive list of publications in educational research.
Examples of Evidence
- Explain how medical education research (carried out internally or obtained from published material) is used to inform your curriculum. Summarise the main themes of this educational research and evaluate the impact of this research on future curriculum development. Provide examples of any medical education research conducted in your own institution.
- Show how your institution promotes excellence in medical education, disseminates good practice, provides a forum for discussion about medical education issues and maintains standards in teaching, learning, assessment and curriculum evaluation. Indicate staff with medical education expertise.
- Please provide your staff/faculty development strategy. Indicate the staff development activities required for key roles e.g. small group teaching, assessment, lecturing. If you operate a peer review system, please provide details.
- Outline your policy for faculty appraisal. Does your institution recognise educational scholarship as a criterion for promotion? Please provide evidence of promotions, based on educational scholarship, which have been successful.
Ready to apply?
Before deciding to submit an application, we recommend that you spend some time discussing the application criteria and required evidence with your team. If you have any questions, please reach out to us prior to submitting your application.
Pricing
The standard charge per submission is £2,500 for each Area of Excellence to be assessed. This is reduced to £2,000 per submission for two or more submissions in the same twelve-month period. The charge for institutions from emerging economies is £1,500 per submission, and £1,250 for two or more submissions in the same calendar year. View the list of emerging economies to see if your institution is eligible. Payment must be received before submissions are sent out for review. Resubmissions are accepted within three years of the original application, with a charge of £2,000 for a resubmission.
Standard Charge
£2,500
Emerging Economies Charge
£1,500
Multiple Standard Submissions
£2,000 per submission
for two or more submissions
in the same twelve-month period.
Multiple Emerging Economies Submissions
£1,250 per submission
for two or more submissions
in the same twelve-month period.
Ready to apply?
Complete the form below to request an invoice.
Glossary
Please note that terms vary from country to country, as does the nature of healthcare delivery. The definitions below are not inclusive and some terms nay be subject to different interpretations in different settings.
Aims – the broad intentions of a programme of study
Appraisal - a regular review of an employee's overall contributions to the institution by his/her manager. Performance appraisals, also called annual reviews, evaluate an employee's skills, achievements and growth, or lack thereof.
Assessment – measurement of students’ progression and achievement of the declared learning outcomes. In the US this is sometimes termed evaluation. Assessment can be written, clinical, oral or computerised.
Blended learning - an education programme that combines online digital media with traditional classroom methods. It requires the physical presence of both teacher and student, with some element of student control over time, place, path, or pace. Blended learning can also be described as the process of mixing introductory didactic lectures, large group case discussions (e.g. clinicopathological cases), self-directed learning using web-based materials etc. with the traditional small group case or problem based process.
Blueprint - a map and a specification for an assessment programme which ensures that all aspects of the curriculum and educational domains are sampled by assessment programmes over a specified period of time. Blueprinting of a specific assessment ensures that the content of the assessment aligns with the learning outcomes of the programme and ensures adequate sampling across subject area and skill domains
Clinical attachment/placement/clerkship - any arrangement in which a student is present in an environment that provides healthcare or related services to patients (medical, dental or veterinary) or the public. Placements can take place in primary, secondary or community healthcare or social care settings. Students can be actively involved in patient care or they can be observing health or social care processes. Examples include: obstetrics and gynaecology ward, community dental practice, livestock farm
Cognitive integration - the facilitation of integrated understanding of the full range of basic and clinical sciences within the mind of the individual learner.
Community – in this context, it simply means outside of a hospital, including people’s homes, schools, community organisations, general practice/family medicine based outside the hospital, rehabilitation centres, community dental surgeries, farms, stables or kennels
Rural/remote community – smaller communities distant from larger centres, e.g. remote Australia outback, the Highlands of Scotland, the rainforests of Malaysia
General Practice / Family Medicine – the work of a doctor based in the community who treats patients with minor and chronic illnesses and refers those with serious conditions to a hospital. General practitioners/family physicians exercise their professional role by promoting health, preventing disease and providing cure, care, or palliation. General Dental Practitioners fulfil similar roles, specialising in oral hygiene and tooth health. A Veterinary Practice is similarly based in the community and deals with disease, disorder and injury in animals
Educational Strategy – the different reasons individual universities have for developing medical, dental or veterinary courses. These are likely to relate to the vision and mission of the school or university. The curriculum is therefore designed to meet particular needs. These may relate, for example, to fulfilling local, national or international health needs, to serving the local community, to the research interests of the faculty or to make up for a shortage of doctors locally or nationally. The educational strategy explains the reasoning behind the educational approaches which have been adopted by the school
Epistemology – By epistemology, we mean the theory or theories of knowledge underpinning the development of the curriculum. Educators’ understanding of the various forms of knowledge and patterns of knowing influence their decisions concerning content selection and its organization during curriculum design and implementation. Selecting an appropriate epistemology based on educational goals, learner development, and context helps shape pedagogy and is important for successful curriculum development.
e-learning - The delivery of a learning, training or education programme by electronic means. e-learning involves the use of a computer or electronic device (e.g. a mobile phone or i-pad) in some way to provide training, educational or learning material.
Elective – an immersive educational experience chosen by the student, that occurs early enough to help the student with career decisions. Learning objectives for the experience are determined by the student and are usually clinical in nature
Evaluation - a systematic method for collecting, analysing, and using information to answer questions about projects, policies and programmes, particularly about their effectiveness and efficiency. Thus evaluation refers to analysis of a programme. In the US, evaluation sometimes means measurement of students’ achievements and progress
External review – a process whereby an institution is subject to external validation of their programmes. This may be by a Statutory Body such as a Medical Council, a Ministry of Education or some other legal entity, or it may simply be an External Examiner appointed by the institution to comment on a programme and its assessments and provide externality and comparability with other similar institutions
Faculty development – courses and workshops for training academic and administrative staff in matters relating to education
Integration
Horizontal integration is where what was once taught in parallel or sequential modules or subjects is taught together as a single module or subject e.g. anatomy, biochemistry, physiology and pharmacology being taught together, alongside sociology, statistics and medical ethics. The common platform for learning could be body systems, life stages or disease categories (see Hays, R 2013 Education for Primary Care 24 151-2)
Vertical Integration is where the basic sciences are integrated with the clinical sciences and clinical practice e.g. clinical skills, diagnosis and management. Commonly, this is achieved through the teaching of clinical and communication skills alongside the basic sciences and case-based/problem based learning
Learning environment - The learning environment includes formal learning activities, the attitudes, values, and informal "lessons" conveyed by individuals who interact with the learners (the hidden curriculum) and the physical spaces where learning takes place.
Shochet, Colbert-Getz & Wright referring to the Johns Hopkins Learning Environment Scale quote: “The medical school learning environment (LE) comprises the physical, social, and psychological contexts in which medical students learn and grow professionally, and it influences how students develop behaviours and form identities as future physicians. The LE encompasses the student’s broadest experience of an academic institution—including the curriculum, the facilities, and interactions with peers, faculty, and staff—as well as the student’s sense of the learning climate, or institutional ethos.”
Objectives – clear and concise statements of what is intended that the student will learn by the end of a programme
Outcomes – broad statements about what the student should be able to do or demonstrate, in terms of knowledge, skills and attitudes by the end of a programme
Pedagogy – the study of how to impart knowledge to students – the science and development of approaches to facilitating learning
Peer review – observation of a teaching event of one member of staff by another (peer) with subsequent constructive feedback on performance. Peer review can sometimes be reciprocal. Students can also take part in peer review.
Patient – member of the public (or animal kingdom) who may utilise the healthcare system
Primary care – the first contact and principal point of continuing care for patients/animals within a healthcare system
Professionalism - a set of values, behaviours, and relationships that underpins the trust the public has in doctors, dentists and vets. All healthcare professionals are committed to integrity, compassion, altruism, continuous improvement, excellence and working in partnership with members of the wider healthcare team. In terms of professional behaviour of students, this includes attendance, punctuality, respect Including respect for equality & diversity) and the practice of sound ethical principles.
Programme - medicine, dentistry or veterinary medicine, in this case
Project - a discrete piece of work conceived with guidance by and for the student. Student choice is the fundamental principle. The project may take several forms e.g. a clinical or laboratory research study, an evaluation of a service or specific intervention, a literature review, an audit, a survey
Quality assurance - the processes by which organisations responsible for education and training demonstrate that their programmes meet the required standards. It includes all the policies, standards, systems and processes that are in place to maintain and improve the quality of medical education and training.
Scholarship/scholarly activity - academic study and achievement at a high level. e.g. by designing and presenting quality courses, developing widely used textbooks or instructional manuals, contributing to regional and national education, publishing research related to education, being recognized by peers as a preeminent scholar, securing extramural funding to develop new curricular tools, and developing distance based learning
Scholarship of teaching and learning should result in work that is communicated publicly such as curriculum development, analysis, and outcomes assessment.
Secondary care – acute care, often but not necessarily in hospitals, for a serious illness, injury or other health conditions
Selective - an immersive educational experience, clinical or non-clinical, that a student chooses from predetermined list. Learning Objectives are usually set by the curriculum or designated committee
Standardised patient
A Standardized Patient (SP) is a person trained to portray the personal history, physical symptoms, emotional characteristics and everyday concerns of an actual patient.
Teaching/learning methodology - Methods of curriculum delivery including, but not limited to, large group teaching, small group teaching (including case based learning, problem based learning and team based learning), self-directed and independent/individualised learning
Case based learning – any learning revolving around patients (including animals) – real, simulated, virtual or paper-based; healthy or ill. This can be in a classroom, in hospital, in the community. It includes problem based learning, bedside teaching, learning in the inpatient setting, in doctors or dentists’ surgeries. It can be individual, in small groups or in large groups
Problem based learning – learning in small groups following a prescribed process, whether short case or progressive release, involving trained facilitators following the Maastricht/McMaster/New Mexico models
Team based learning – a structured, student-centred learning and teaching strategy designed to promote active learning through a process of preparation, testing and application of knowledge. The learning takes place in teams of 5-7 students
Self-directed learning – individual students take the initiative, with or without the assistance of others, in diagnosing their learning needs, formulating learning goals, identifying learning resources, choosing and implementing appropriate learning strategies and evaluating learning outcomes.
Independent or Individualised learning – learning on one’s own, but with prescribed resources, tasks etc. Individual project work or electives would come into this category, for example